Abstract
Background: During pregnancy profound immunologic, metabolic, endocrine and vascular changes occur resulting in both physiologic and pathologic changes in the skin and its appendages. These skin changes can be separated into three main categories namely hormone related, pre existing and pregnancy specific.
Aim: The present study was conducted with an aim to find the clinical pattern and incidence of various skin changes of pregnancy.
Methods: All pregnant females reporting to antenatal clinic of SGT Medical College and Hospital during the period of one year were included in this study.
Results: A total of 341 pregnant women were enrolled in the present one year long study out of which 194 (56.89%) were primigravidas and 147 (43.11%) were multi gravidas. Maximum incidence of 78% was found in the age group between 15-25 years of age. Physiological changes were seen in all the pregnant females while dermatoses affected by pregnancy were reported in only 12.3% cases. Dermatoses specific for pregnancy were found in 7.9% cases.
Conclusion: Clinicians must be able to distinguish physiological changes of pregnancy from several other dermatoses that can present during the period of pregnancy in order to provide timely management and thus reducing maternal and fetal morbidity.
Keywords: pregnancy, dermatoses, skin
Introduction:
Cutaneous changes and eruptions during pregnancy are exceedingly common and in some cases a cause for substantial anxiety on the part of the prospective mother. Some of these are benign and reversible after delivery whereas others can have potential effects on foetus in terms of morbidity and mortality.[1] Likewise, The concerns of the patient may range from cosmetic appearance, to chance of recurrence of the particular problem during a subsequent pregnancy, to its potential risks on fetus.[2] There are three general categories of pregnancy associated skin conditions: 1) benign skin conditions from normal hormonal changes or physiological skin changes, 2) pre existing skin conditions that change during pregnancy or skin diseases affected by pregnancy, and 3) pregnancy specific dermatoses.[3] Physiological skin changes include striae gravidarum, hyper pigmentation and hair, nail and vascular changes. Pre existing skin conditions that may be affected by pregnancy include psoriasis, atopic dermatitis, candidal and other fungal infections, benign appendageal lesions and many more. True dermatoses of pregnancy include pruritic urticarial apples and plaques of pregnancy (PUPPP), prurigo of pregnancy, intrahepaticcholestasis of pregnancy, pemphigus gestationis, impetigo herpetiformis and pruritic folliculitis of pregnancy.
Materials and Methods:
The study comprised all pregnant females reporting to antenatal clinic of SGT Medical College and Hospital during the period between January 2015 to December 2015 were included in this study. A total of 346 pregnant women were included in the study. Informed consent was obtained before before the interview and clinical examination.
All patients were subjected to detailed history and thorough clinical examination to note all the physiological and pathological mucocutaneous changes. Routine blood, urine and stool examination, and screening with VDRL and ELISA for HIV was done in all cases. In patients with white discharge, a KOH mount, saline mount and gram stain were done.
Results:
A total of 341 pregnant females were included in the one year study conducted between January 2015 to December 2015. Patients were divided in age groups between 15-25 years (266 cases, 78%) and 26-40 years (75 cases, 22%). Of these, 194 (56.89%) females were primigravidas and 147 (4.11%) were multi gravidas. Most of them presented in their third trimester (222, 65.1%) followed by second (75, 22%) and first trimester (44, 12.9%).
Pruritus was the commonest symptom reported accounting for 18.2% (62) of the patients, followed by white discharge per vagina (21, 6.1%), while few complained of presence of one or other type of skin lesions due to dermatoses which were broadly divided into three categories:
Physiological cutaneous changes Skin diseases (Pre existing or newly occurring) affected by pregnancy.
Pregnancy specific dermatological disorders.
Physiological changes were seen in 100% of cases, while dermatoses modified by pregnancy were observed in 12.3% cases and only 7.9% had dermatoses specific for pregnancy.
Among the physiological changes, most common were the pigmentary changes including lineanigra, areolar pigmentation and melasma followed by connective tissue changes mainly including striae gravidarum.[Table 1]
Candidal vaginitis (13, 3.81%) was found to be the most common dermatosis affected by pregnancy closely followed by acne vulgaris (9, 2.64%) and eczemas (6, 1.76%).[Table 2]
Total of 37 females were diagnosed of pregnancy specific dermatoses of which 19 (5.57%) had PUPPP (pruritic urticarial papules and plaques of pregnancy).[Table3]
Discussion:
Pruritus was reported to be the commonest symptom with incidence of 18.2% in the present study. According to Winton et al, pruritus from all cases may occur in 17% of pregnant women,[4] while Wong et al and Roger et al reported incidence of pruritus in 20% and 18% respectively.[5,6]
Candidal vaginitis was found to be the most common cause for vaginal discharge. That monilial vaginitis is 10 to 20 times more common during pregnancy has been supported by Winton et al and Dotz et al.[1,7]
Physiological changes were seen in all the pregnant females. Several other studies have reported physiological changes in upto 100% cases.[8,9] Pigmentary changes were noticed in all the cases.[3] Striae were found to be the commonest physiological change (87.68%) closely followed by Lineanigra (85.3%) and areolar hyper pigmentation (82.1%) [Fig 2]. Other less commonly encountered physiological changes were melasma, gingivitis, acne, montgomery tubercles, hair and nail changes.
The most common physiological changes are pigmentary alterations, stretch marks, vascular spiders and telogen effluvium.[10] Pigmentary changes occurred in 98.82% of the patients.[11] Similar incidences have been reported by other authors.[4,5,7] Incidence of melasma was reported to be 10% similar to the finding of V. Shivakumar and Raj et al.[11,12]
In our study, striae gravidarum were seen in 299 (87.68%) cases. A few studies have shown incidences between 60 to 80% [8,9,11,12] while others have reported incidences upto 90%.[1,5,7]
Montgomery’s tubercles is well known during pregnancy in 30-50% of pregnant women. [10] In our study, Montgomery’s tubercles were seen in 22 (6.45%) cases. This was found to be consistent with other studies. [13]
Vascular changes result from distension, instability and proliferation of vessels [4] and were seen in 45.16 % of cases. Non pitting edema over the hands, feet and face was observed in 35.78% cases. Muzaffer et al [8] reported edema in 48.5% whereas Rashmi et al [9] reported it in 9.8%. Varicosities were seen in 1.17% comparable to other studies. [8,12]
Gingivitis may occur in upto 100% of pregnant women with varying degree of severity.[5] 6.15% cases of gingivitis were reported. A bit higher percentage has been reported by other authors.[8,13]
PUPPP (also known as polymorphic eruption of pregnancy) was the commonest specific disorder of pregnancy accounting for 5.57% followed by prurigo of pregnancy with 12 (3.52%) cases and pruritus gravidarum (also known as intrahepaticcholestasis of pregnancy) with 4 (1.17%) cases. Similar to our study, PUPPP was reported as commonest specific dermatoses of pregnancy in study by Kumari R [9] accounting for 63.6% cases followed by pruritus gravidarum while Shivakumar and Madhavamurthy [11] reported prurigo of pregnancy as the commonest specific dermatoses of pregnancy with incidence of 9.41% followed by pruritus gravidarum.
Conclusion:
To conclude, a variety of cutaneous lesions can be seen in pregnant women which need a meticulous examination and investigations to reach a correct diagnosis enabling careful management in an effort to minimise maternal and foetal morbidity.
References:
- Kroumpouzos G, Cohen LM. Dermatoses of pregnancy. J Am Acad Dermatol 2001;45:1-19. [PUBMED] [FULLTEXT]
- Lawley TJ, Yancey KB. Skin changes and diseases in pregnancy. In: Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, et al , editors. Fitzpatrick’s Dermatology in general medicine. 5th ed. McGraw-Hill: New York; 1999. p. 1963 9.
- Marc Tunzi, Gary R. Gray. Am Fam Physician. 2007 Jan 15;75(2):211-218.
- Winton GB, Lewis CW. Dermatoses of pregnancy. J Am Acad Dermatol 1982;6:977 998. [PUBMED] [FULLTEXT]
- Wong RC, Ellis CN. Physiologic skin changes in pregnancy. J Am Acad Dermatol 1984;10:929-940. [PUBMED] [FULLTEXT]
- Roger D, Vaillant L, Fognon A, et al. Specific pruritic diseases of pregnancy. Arch Dermatol 1994;130:734-739.
- Dotz W, Berman B. Dermatologic problems of pregnancy. In: Cherry SH, Merkatz IR, editors. Complications of Pregnancy: Medical Surgical Gynaecologic Psychosocial and Perinatal, 4th ed. Baltimore : Williams and Wilkins, 1991:562 587. Back to cited text no. 6
- Muzaffar F, Hussain I, Haroon TS. Physiologic skin changes during pregnancy: A study of 140 cases. Int J Dermatol 1998;37:429-31.[PUBMED]
- Kumari R, Jaisankar TJ, Thappa DM. A clinical study of skin changes in pregnancy. Indian J Dermatol VenereolLeprol 2007;73:141.
- Martin AG, Leal-Khouri S. Physiological skin changes associated with pregnancy. Int J Dermatol 1992;31:375-8.
- Shivakumar V, Madhavamurthy P. Skin in pregnancy. Indian J Dermatol VenereolLeprol 1999;65:23-5.
- Raj S, Khopkar V, Kapasi A, et al. Skin in pregnancy. Indian J Dermatol VenereolLeprol 1992;58:84-88.
- Rathore SP, Gupta S, Gupta V. Pattern and prevalence of physiological cutaneous changes in pregnancy: A study of 2000 antenatal women. Indian J Dermatol VenereolLeprol 2011;77:402.

* more than one dermatoses were present in many cases
Table 1: physiological changes of pregnancy
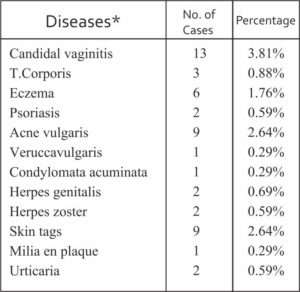
Table 2: Dermatoses affected by pregnancy
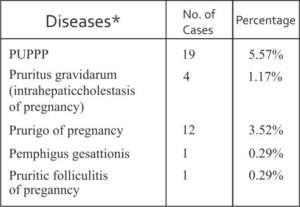
Table 3: pregnancy specific dermatoses
*-*-*




