Exogenous Ochronosis (EO) is avoidable dermatitis, on the rise cause of unjustified use of topical hydroquinone; it is mainly encountered in melasma patients on triple therapy and is turning out to be a menace cause of difficulty in its treatment. Phenol is also known to a cause the condition.
Pathologically, a microscopic deposition of yellow (ocher-colored) pigment is found in the dermis. It is clinically and histopathologically similar to endogenous Ochronosis, also known as alkaptonuria; difference between them is that it does not present systemic manifestations such as history of dark urine, gray-blue or gray-brown coloration of cartilages, conjunctive and arthropathy and the affected area is limited to that treated with HQ.
In 1912Berddard and Plumtre described an EO case in a patient that had used phenol to treat a lower limb ulcer.In 1975 Findlay described the first EO case related to HQ,
Frequently used for the treatment of melasma, hydroquinone interferes in skin pigmentation through alteration of melanin formation, interaction with copper at the site of tyrosinase activity and in inhibition of DNA and RNA synthesis.
Hydroquinone in hydro alcoholic solution, which has a significantly higher penetration in the skin, is also an important contributing factor for EO development.
GRADING
In 1989, Hardwick et al.[41] in their epidemiological study based on clinical diagnosis graded EO as:
- Grade I – Faint macular sooty pigmentation
- Grade II – Distinct macular stippling/small papules
- Grade III – Dark deposits and papules
- Grade IV – Colloid milia (1 mm and greater) [Figure 4]
- Grade V – Keloid‑like nodules and cysts.
SYMPTOMS
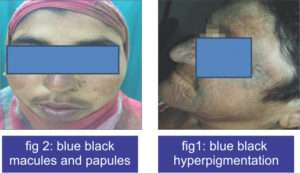
- yellow-brown, banana-shaped fibers
- caviar-like papules
- brown-grey or blue-black hyper-pigmentation
The majority of the lesions will be seen on areas of the body that get the most sun.
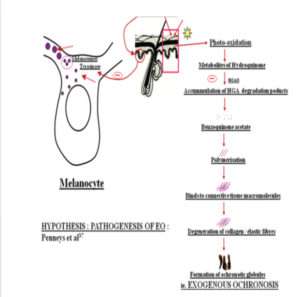
Pathogenesis of Ochronosis
TREATMENT
Exogenous Ochronosis is not easy to treat therefore prevention is extremely important.
- Avoiding the causative agent of the disease.
- The use of lower HQ concentrations.
- Sun protection.
- Early diagnosis of irritation.
- Suspension of treatment in case there is no clinical improvement within six months.
Treatment modalities
- Sunscreens are extremely beneficial in limiting further augmentation of the condition.
- Glycolic acid peelings.
- Retinoic acid gives appreciable improvement.
- Low potency corticosteroids in association with photo protection.
- Dermoabrasion.
- CO2 laser and Q-switched laser.
However, the results are not uniform and this condition continues to be of difficult treatment.
Hence, Hydroquinone prescription should be associated with full knowledge of side effects and orientation about proper use, to prevent the occurrence of this cosmetically disfiguring condition.
REFRENCES
- Tan SK, Sim CS, Goh CL. Hydroquinone-induced exogenous ochronosis in Chinese – two case reports and a review. Int J Dermatol. 2008;47:639-40.
- Online Etymology Dictionary. Available from :http://www.etymonline.com. [Last accessed on 2013 oct 06].
- Longo N. Inherited disorders of amino acid metabolismpresenting in adults. In: Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL, editors. Harrison’s Principles of Internal Medicine. 15th ed. New York: McGraw Hill; 2001.p. 2307.
- Zawar VP, Mhaskar ST. Exogenous ochronosis following hydroquinone for melasma. J CosmetDermatol. 2004;3:234-6.
- Fisher AA, Davis MW. Alkaptonuricochronosis with aortic valve and joint replacements and femoral fracture: A case report and literature review. Clin Med Res 2004;2:209‑ Laskar FH, Sargison KD. Ochronoticarthropathy. J Bone Joint Surg 1970;52:653‑66.
- Tharini G, Ravindran V, Hema N, Prabhavathy D, Parveen B. Alkaptonuria. Indian J Dermatol 2011;56:194‑
- Bongiorno MR, Aricò M. Exogenous ochronosis and striaeatrophicae following theuse of bleaching creams. Int J Dermatol. 2005;44:112-5.
- Charlín R, Barcaui CB, Kac BK, Soares DB, Rabello-Fonseca R, Azulay-Abulafia L.Hydroquinone-induced exogenous ochronosis: a report of four cases and usefulness of dermoscopy. Int J Dermatol. 2008; 47:19-23.




